Selective Internal Radiotherapy (SIRT) of hepatic malignancies and liver metastases
How does SIRT work?
Selective Internal Radiotherapy (SIRT) is a targeted internal radiation therapy of malignant tumours and metastases in the liver (radioembolization). Microscopically small particles (microspheres) which are loaded with a radioactive substance are injected into the hepatic artery. The microspheres accumulate in the tumour tissue, which receives blood flow from this artery (embolization). Due to the short range of the therapeutically active radiation in the tissue (beta-radiation), the tumours are irradiated with high efficacy while mostly sparing the surrounding normal liver tissue. SIRT can reduce the size of the tumours or even completely eradicate the tumours.
In which cases can SIRT be performed?
Primary liver tumours (hepatocellular cancer, HCC, and intrahepatic cholangiocellular cancer CCC) and secondary liver tumours (liver metastases of other tumours such as colorectal cancer, neuroendocrine tumours, breast cancer and melanoma) can be treated with SIRT. It is indicated when surgery, chemotherapy, medical therapy and other targeted forms of liver therapy (e.g. RFA, MWA, TACE, etc.) has not been effective or are not possible to perform. As SIRT does not target tumour lesions outside the liver, it is only indicated if the tumour burden is dominantly located in the liver.
It is important to note that SIRT is a palliative form of treatment, which may prolong the life of patients, but in most cases, it cannot completely cure the tumour disease. In some cases, a reduction of tumour size by SIRT can enable surgical removal of initially inoperable tumours.
The indication for SIRT needs to be decided in an interdisciplinary tumour board focused on gastrointestinal malignancies, which takes place in our institution on a regular basis. The patient’s treating physician should initiate the application for SIRT in our institution. It is highly recommended that all patients receive oncological co-treatment and tight follow-up by an oncologist or an oncological centre after SIRT has been performed.
How long have radioembolizations been performed in Bonn?
Targeted therapy of liver tumours using radionuclides has been performed in our clinic in cooperation with the department of radiology already as early as 1998.
SIRT is performed by a team of nuclear medicine physicians and radiologists.
Pre-interventional diagnostics
For therapy planning, up-to-date imaging studies of the liver (e.g. CT, MRI, PET/CT) are required to evaluate tumour extent in the liver and exclude relevant tumour burden in other organs except from the liver.
After an initial review of the imaging studies, a simulation study is performed using a diagnostic radiotracer (Tc-99m-MAA). The simulation study is performed during an inpatient stay of about 2 days. During an angiographic exam, the arterial feeds to the liver and to the tumour are assessed. Arteries leading to organs outside the liver might be occluded (coiled) during this exam to prevent accumulation of the radioactive particles in organs other than the liver. Then the diagnostic tracer (Tc-99m-MAA) is injected in the liver artery in a similar way as if SIRT was performed and scintigraphic images are acquired with a gamma-camera (SPECT/CT, see figure 1). This is done to assess tracer uptake in the tumour lesions relative to normal liver tissue and to exclude tracer accumulation in other organs than the liver (see figure 2). One day later, patients can be discharged from the ward and SIRT therapy is planned to take place in the 2 weeks following the simulation study.
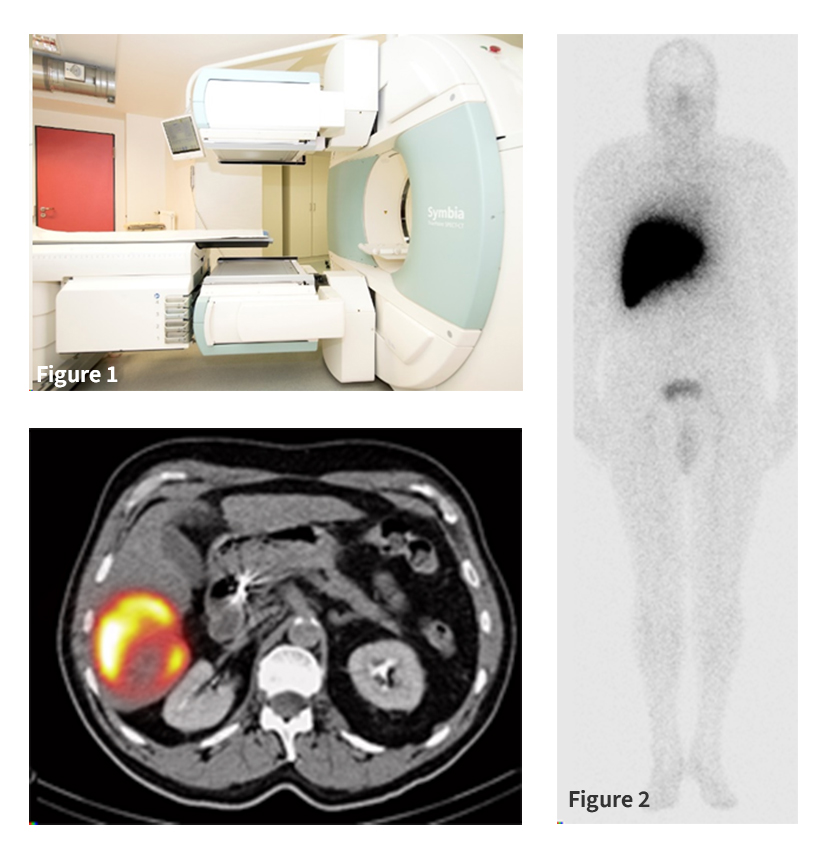
Figure 1: SPECT/CT
Figure 2: Left: Whole body scintigraphy after application of the diagnostic tracer Tc-99m-MAA into the right liver artery. Right: SPECT/CT images of Tc-99m-MAA accumulation in the tumour in the right liver lobe.
Up to 2 weeks after the pre-interventional diagnostics (Tc-99m-MAA study), patients come to our inpatient therapy ward for 2-3 days for SIRT. Fasting is required on the day before SIRT. The SIRT procedure is similar to the simulation study, with the exception that instead of the diagnostic tracer (Tc-99m-MAA) the therapeutically active radioactive microspheres (loaded with the beta-emitter Yttrium-90) are injected into the liver artery. The radioactive microspheres then remain implanted in the tumour tissue. The radioactivity decays with a physical half-life of 64 hours and by this manner, therapeutically effective radiation doses can be applied to the tumour, killing the tumour cells while the surrounding healthy tissue is mostly spared from the radiation. Depending on the size and location of the tumour lesion(s), only one or both lobes of the liver are treated.
After SIRT, patients need to stay on the inpatient ward for 48 hours due to radiation safety regulations. During this period, scintigraphic images of the liver are acquired after therapy to document the successful delivery of the microspheres to the targeted tumour tissue and to exclude activity accumulation in organs outside of the liver (see figure 3). On discharge, patients receive a detailed therapy report. After SIRT, regular physical examinations and follow-up imaging studies (e.g. CT, MRI, PET/CT) will be necessary.
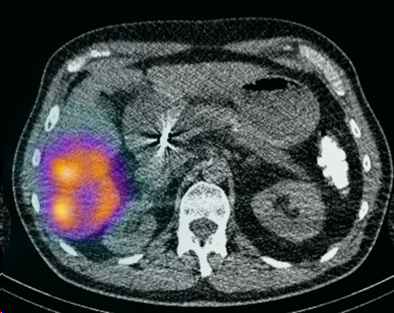
Figure 3: Scintigraphic images (SPECT/CT) after successful implantation of the therapeutically active Yttrium-90-labeled microspheres in the tumour tissue in the right liver lobe.
In general, SIRT is tolerated well by most patients. Shortly after implantation of the SIRT microspheres, some patients might experience abdominal pain in the liver region, nausea or fever, provoked by the embolization of small liver arteries. These symptoms are temporary, self-limiting and can be generally controlled well by suitable medication.
SIRT is a very safe treatment in the hands of experienced physicians. Severe side effects are rare. These might occur when the SIRT microspheres deviate from the liver vessels and are transported to other organs outside the liver, e.g. to the stomach, which can lead to stomach ulcers. In case of a reduced functional reserve of the liver, a radiation-induced inflammation of the liver tissue might occur, leading to further impairment of the liver function. In rare cases, significant shunts from the liver to the lungs can lead to accumulation of the microspheres in lung tissue, leading to inflammation of the lung tissue (radiation-induced pneumonitis).
You can reach us
Therapy secretary office / enquiries
Mrs. Oregan Vautey
Tel: +49 (0)228 287 16171
Email:
Online appointment form
Therapy Ward
Tel: +49 (0)228 287 16855
Fax: +49 (0)228 287 19107








